Hit enter to search or ESC to close
A medial to lateral approach is generally the preferred approach unless the surgeon is unable to safely identify the anatomy. This approach allows the surgeon to safely separate the left colonic mesentery from the retroperitoneum and protect the ureter, retroperitoneal blood vessels, and sympathetic nerves. The exposure is facilitated by reflecting the small bowel out of the pelvis. This is accomplished with a combination of Trendelenburg positioning and rotating the bed with the right side down.
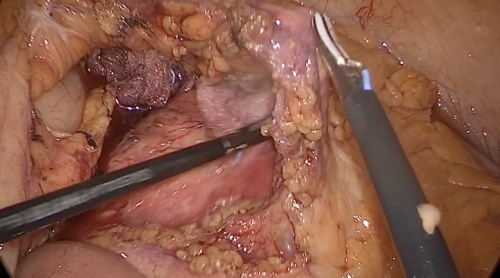
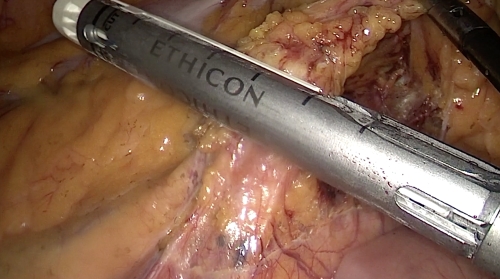
We can identify the sacral promontory, and the inferior mesenteric artery (IMA) pedicle from this view. Once the pedicle is placed on a gentle stretch, a mesenteric window is created with cautery. The pedicle is lifted upwards and a gentle blunt dissection in the proper congenital fusion plane between the mesentery and retroperitoneum. Once the mesentery is lifted off the retroperitoneum, the left ureter and gonadal vessels are swept away from the pedicle. We prefer an energy device to transect the mesentery. The surgeon should have a grasper ready to gently occlude the pedicle, should it bleed, thus allowing a controlled application of an endoloop/clip if necessary.
Sigmoid colon mobilizationIf the dissection was done correctly from the medial approach, there should not just be a purple and thin appearance to the peritoneum laterally. The colon is grasped with an atraumatic bowel grasper and retracted medially. The colon is mobilized off the retroperitoneum by dissecting through this thin peritoneal layer. The abscess was drainend. The location of the ureter, gonadal vessels and iliac vessels are confirmed and the sigmoid colon is mobilized until it is a midline structure. In the same manner, the remainder of the descending colon is mobilized off the lateral retroperitoneal attachments.
Splenic flexure mobilizationIn many instances, simple mobilization of the descending colon is not enough to achieve a tension free anastomosis. In this case, the splenic flexure should be mobilized, and this can easily be accomplished laparoscopically. Typically, the lateral dissection continues, rolling the colon mesentery medially away from Gerota’s fascia over the kidney. The renocolic, splenocolic, and phrenicocolic attachments are released. The gastrocolic ligament is then taken down to enter the lesser sac and mobilize the omentum off the transverse colon until the midline or middle colic vessels are reached depending on the indication for the operation. If the colon still does not reach, ligation of the IMV near the inferior border of the pancreas may be needed, but this is rarely necessary outside of low rectal cancer surgery.
Distal transectionLastly, the remaining peritoneal attachments are divided, taking care to protect both ureters and the sympathetic nerves at the sacral promontory. An energy device is used to thin out the rectal mesentery to prepare the rectum for a transection. The rectum is transected with a laparoscopic linear cutter stapler, ideally in one single firing
A Pfannenstiel incision for extraction is preferred due to its lower risk of incisional hernia formation and wound complications. The colon is then exteriorized and the proximal transection margin is identified. The anvil of an EEA stapler is inserted into the proximal cut end and secured with a purse string. The colon is placed back into the abdomen and insufflation is reestablished. An assistant inserts an EEA stapler into the anus and up to the apex of the rectal segment. The anvil is then docked onto the spike. It is important to confirm correct orientation of the colon by using the cut edge of the mesentery. The stapler is then closed, fired and removed. The stapler “donuts” are removed and examined to ensure an intact staple line. Finally, a leak test is performed by filling the pelvis with water and performing sigmoidoscopy to ensure an airtight anastomosis
After the leak test, the abdomen is irrigated and adequate hemostasis is confirmed. Pneumoperitoneum is allowed to deflate and the 12 mm port site is closed in a figure-of-eight fashion. The skin is closed with interrupted, absorbable sutures.
Ospedale Arnas Garibaldi Centro – Catania
Utilizziamo i cookie per rendere il nostro sito più facile ed intuitivo. I dati raccolti grazie ai cookie servono per rendere l’esperienza di navigazione sempre efficiente in futuro.
Cosa sono i cookie?
I cookie sono piccoli file di testo inviati dal sito al terminale dell’interessato (solitamente al browser), dove vengono memorizzati per essere poi ritrasmessi al sito alla successiva visita del medesimo utente. Un cookie non può richiamare nessun altro dato dal disco fisso dell’utente né trasmettere virus informatici o acquisire indirizzi email. Ogni cookie è unico per il web browser dell’utente.
Alcune delle funzioni dei cookie possono essere demandate ad altre tecnologie. Nel presente documento con il termine ‘cookie’ si vuol far riferimento sia ai cookie, propriamente detti, sia a tutte le tecnologie similari.
Tipologia dei cookie
I cookie possono essere di prima o di terza parte, dove per “prima parte” si intendono i cookie che riportano come dominio il sito, mentre per “terza parte” si intendono i cookie che sono relativi a domini esterni.
I cookie di terza parte sono necessariamente installati da un soggetto esterno, sempre definito come “terza parte”, non gestito dal sito. Tali soggetti possono eventualmente installare anche cookie di prima parte, salvando sul dominio del sito i propri cookie.
Un altro tipo di cookie sono i cosiddetti “Flash Cookie” (Local Shared Objects), utilizzati all’interno di Adobe Flash Player per erogare alcuni contenuti, come video clip o animazioni, in modo da ricordare le impostazioni e preferenze. I Flash cookie sono archiviati sul dispositivo, ma sono gestiti attraverso un’interfaccia differente rispetto a quella fornita dal browser utilizzato.
Natura dei cookie
Relativamente alla natura dei cookie, ne esistono di diversi tipi:
Cookie tecnici
I cookie tecnici sono quelli utilizzati al solo fine di “effettuare la trasmissione di una comunicazione su una rete di comunicazione elettronica, o nella misura strettamente necessaria al fornitore di un servizio della società dell’informazione esplicitamente richiesto dall’abbonato o dall’utente a erogare tale servizio” (cfr. art. 122, comma 1, del Codice).
Essi non vengono utilizzati per scopi ulteriori e sono normalmente installati direttamente dal titolare o gestore del sito web. Possono essere suddivisi in:
• cookie di navigazione o di sessione, che garantiscono la normale navigazione e fruizione del sito web (permettendo, ad esempio, di realizzare un acquisto o autenticarsi per accedere ad aree riservate); essi sono di fatto necessari per il corretto funzionamento del sito;
• cookie analytics, assimilati ai cookie tecnici laddove utilizzati direttamente dal gestore del sito per raccogliere informazioni, in forma aggregata, sul numero degli utenti e su come questi visitano il sito stesso, al fine di migliorare le performance del sito;
• cookie di funzionalità, che permettono all’utente la navigazione in funzione di una serie di criteri selezionati (ad esempio, la lingua, i prodotti selezionati per l’acquisto) al fine di migliorare il servizio reso allo stesso. Per l’installazione di tali cookie non è richiesto il preventivo consenso degli utenti (più informazioni nel paragrafo Gestione dei cookie in basso).
Cookie di profilazione
I cookie di profilazione sono volti a creare profili relativi all’utente e vengono utilizzati al fine di inviare messaggi pubblicitari in linea con le preferenze manifestate dallo stesso nell’ambito della navigazione in rete. Per l’utilizzo dei cookie di profilazione è richiesto il consenso dell’interessato.
.
1 review for Sit voluptatem
admin - November 22, 2018
Good Product